How can concepts from financial economics strengthen conventional health economic methods for evaluating programs that reduce system-level risk?
Conventional health economic evaluations (HEE) are powerful, but are we systematically underestimating the value of our most critical public health programs – like disease elimination and eradication?
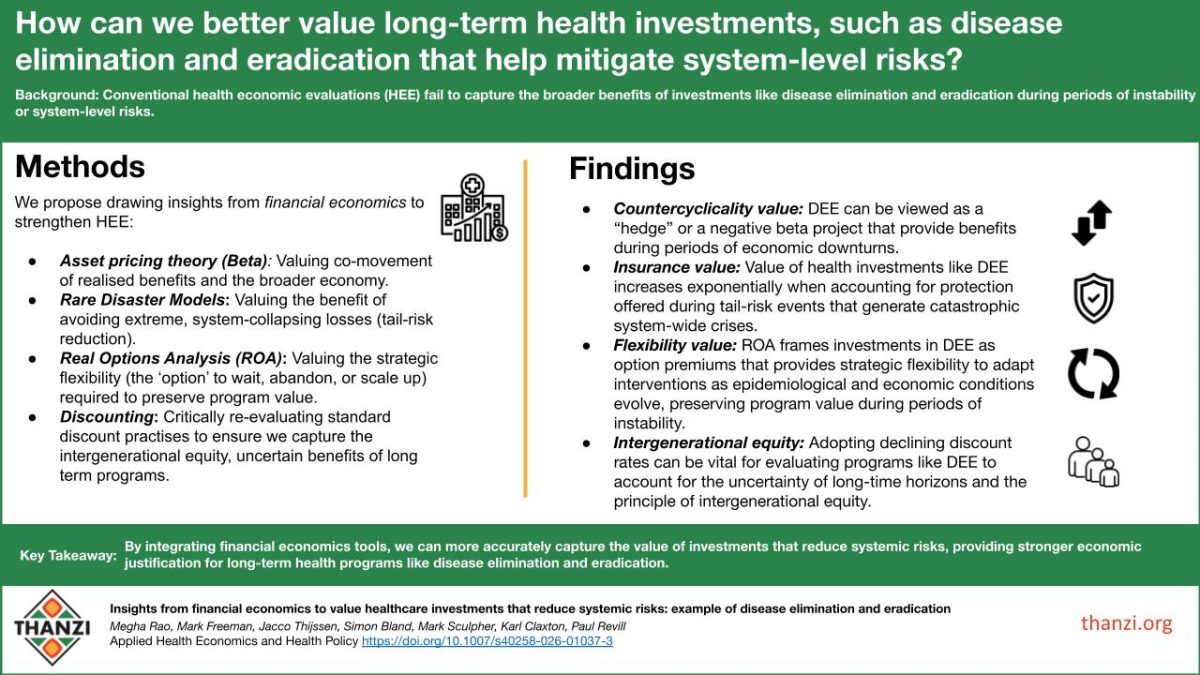
Our latest paper – ‘Insights from financial economics to value healthcare investments that reduce system-level risks: example of disease elimination and eradication’ – suggests that current models often overlook crucial benefits these programs provide during system-level risks. This is particularly relevant for policymakers and resource-allocation specialists in LMICs, where fragile systems face greater risks of instability and extreme events.
Conventional HEE assumes a ‘steady-state’—ignoring the potential value generated when these investments reduce the aggregate impact of system-level risks like pandemics or economic crises. To ensure we achieve ‘more health for the money’, we must adopt advanced financial tools to capture this broader value.
“The current health economics toolkit is arguably more tailored to quantify and determine the impact of intervention-specific risks under normal circumstances, while neglecting broader impacts on healthcare system demand and supply during periods of severe stress or resource constraints.”
This paper proposes integrating methods from financial economics to strengthen the evaluation of health investments that build system resilience.
Key Insights:
- Valuing countercyclicality – Health programs like DEE exhibit countercyclical benefits, functioning as negative beta assets that provide protection during downturns. Accounting for this countercyclical value would likely strengthen the economic case for such investments.
- Valuing insurance function – Programs like DEE provide critical insurance against disease re-emergence during catastrophic tail-risk events. Though rare, these coincident crises generate enormous system-wide losses, making such investments valuable insurance policies that warrant higher priority in resource allocation.
- Valuing Strategic Flexibility via Real Options: ROA frames investments in DEE like early warning systems as option premiums that provide policy-makers with strategic flexibility to adapt interventions as epidemiological and economic conditions evolve, preserving program value during periods of instability.
- Valuing intergenerational equity: The paper suggests scrutinising the use of standard, fixed discount rates for very long-term programs like DEE, whose benefits span multiple generations. Aligning discounting practices with the broader social objectives of equity can help ensure the very long-term, uncertain benefits of elimination and eradication are valued appropriately.
By integrating these insights into economic evaluation methods, we aim to strengthen the analytical frameworks that inform health policy decisions, particularly by identifying where conventional approaches may undervalue systematic and systemic risk reduction benefits. This methodological strengthening can support more informed resource allocation decisions for long-term health investments. in Africa and globally.
“The financial economics tools highlighted here could serve as key components of a broader analytical framework, supporting investment decisions that recognise and more accurately capture the value of investments that reduce the aggregate impact of system-level risks.”
Link to open access article in Applied Health Economics and Health Policy: Insights from Financial Economics to Value Healthcare Investments that Reduce System-Level Risks: Example of Disease Elimination and Eradication. Authors: Megha Rao, Mark Freeman, Jacco Thijssen, Simon Bland, Mark Sculpher, Karl Claxton, Paul Revill.
By: Kath Devlin & Megha Rao | March 2026


{kind=link}
{kind=link}
{kind=link}